Bone Healing Risk & Outcome Estimator
Fracture Details
Patient Risk Factors
Select any factors that apply to the patient.
Analysis Result
Select options and click Estimate to see your analysis.
You break a bone. You cast it. You wait. But sometimes, the pain just doesn't go away. Or worse, the X-ray shows that the break has never actually closed up. It sounds like a nightmare, but for some specific fractures, this isn't just bad luck-it's biology. When people ask which bone never heals, they are usually referring to a specific anatomical reality rather than a magical curse. The answer is complex, but one bone stands out in medical literature for its notorious difficulty in achieving true union: the fibula, specifically at certain attachment points.
It’s not that the fibula refuses to heal entirely. If you snap the shaft of your lower leg, it will knit back together. But if you tear off a small piece of bone where a tendon attaches-an avulsion fracture-that fragment often stays loose forever. And that’s okay. In fact, it’s usually the best outcome. This counterintuitive truth challenges everything we think about broken bones and recovery.
The Myth of the "Unhealable" Bone
We are taught from childhood that bones are resilient. They break, they hurt, and then they fix themselves better than before. This is true for most skeletal injuries. However, the human body is not a uniform machine. Different parts have different blood supplies, different mechanical stresses, and different biological instructions.
When doctors talk about a bone that "never heals," they are rarely talking about a long bone like the femur or tibia failing to unite (a condition called non-union). While non-unions do happen-often due to smoking, diabetes, or severe trauma-they are exceptions, not the rule. The real story lies in the avulsion fracture. This occurs when a muscle or tendon pulls so hard during a sudden movement that it rips a chunk of bone away from the main structure.
In many cases, particularly with the fibula, that little chip of bone does not reattach. It becomes a free-floating fragment inside the joint or soft tissue. Yet, patients often walk away without permanent disability. Why? Because the body adapts. The tendon scar-tissues over the gap, creating a functional bridge even though the bony connection remains severed. The bone didn't heal, but the function returned.
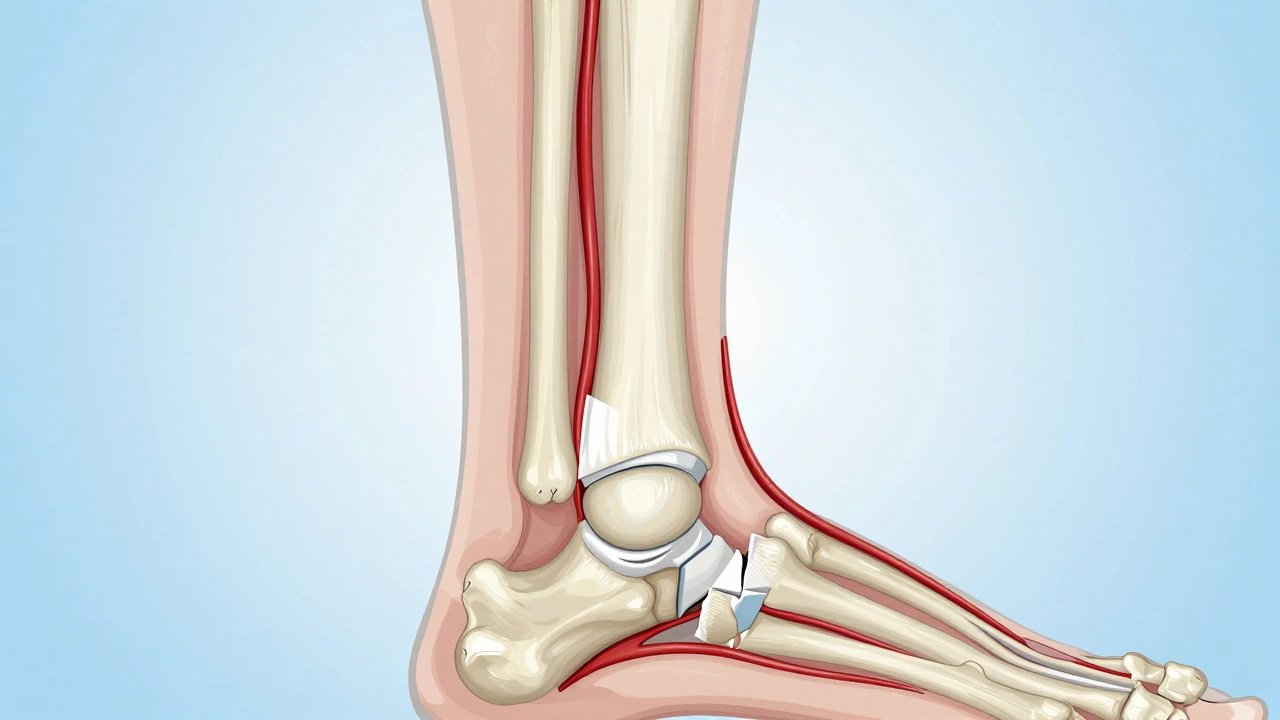
Why the Fibula Is Unique
To understand why the fibula gets this reputation, we need to look at what it actually does. Most people assume both shin bones carry equal weight. They don’t. The tibia carries about 85% to 90% of your body weight. The fibula carries only about 10%. Its primary job isn't weight-bearing; it’s stability. It anchors the ankle joint and provides attachment points for muscles.
Because the fibula is thin and subjected to high tensile forces from powerful calf and thigh muscles, it is prone to those avulsion tears. Imagine pulling a rope tied to a wall. If the rope is stronger than the paint on the wall, the paint peels off. That’s an avulsion fracture. The tendon (rope) is strong; the bone surface (paint) is weak.
When this happens at the lateral malleolus-the bony bump on the outside of your ankle-the fragment often sits in a position where surgical removal is risky, but leaving it causes no pain once the acute inflammation subsides. Surgeons frequently choose to leave these fragments alone. They become "non-unions" by design. The body accepts them as permanent residents.
Blood Supply: The Secret Ingredient
If you want to know why some bones heal and others don’t, look at the blood flow. Bone is living tissue. It needs oxygen and nutrients to repair itself. Without adequate blood supply, dead bone cells accumulate, and healing stalls. This is known as avascular necrosis.
The scaphoid bone in the wrist is another famous example of a bone that struggles to heal. It has a retrograde blood supply, meaning blood flows into it from the distal end and works backward. If you break the proximal pole of the scaphoid, you cut off the blood supply to the larger fragment. Without blood, that piece dies. It literally cannot heal because the cellular machinery required for repair is starved.
While the fibula generally has decent blood flow, the specific areas involved in avulsion fractures are often covered by cartilage or synovial fluid, which inhibits direct bone-to-bone contact. Cartilage does not bleed. Therefore, two pieces of bone separated by cartilage or joint space will never fuse naturally unless surgically forced together.
| Bone Location | Common Injury Type | Healing Difficulty | Primary Reason |
|---|---|---|---|
| Fibula (Avulsion) | Tendon pull-off | High (Non-union common) | Functional tolerance; fragment left alone |
| Scaphoid (Wrist) | Proximal pole fracture | Very High | Avascular necrosis (poor blood supply) |
| Tibia Shaft | Comminuted fracture | Moderate | Soft tissue damage and infection risk |
| Patella (Kneecap) | Transverse split | Low (with surgery) | High tension from quadriceps |
When "Not Healing" Is Actually Good
This is the part that confuses most patients. We equate "healed" with "fixed." But in orthopedics, "functional" is the goal, not necessarily "anatomical perfection." If a small fragment of the fibula remains unattached, but your ankle is stable and pain-free, the treatment was successful.
Sometimes, trying to force a bone to heal causes more problems. Surgery introduces infection risks, nerve damage, and longer recovery times. For a tiny avulsion fragment, the cost of surgery outweighs the benefit. The body forms a scar tissue bridge. This scar tissue is strong enough for daily activities, even if it’s not bone. You might see a gap on an X-ray years later, but you won’t feel it.
Consider the olecranon bursa in the elbow. Sometimes, chronic irritation leads to calcification. These calcium deposits never "heal" or disappear; they just sit there. Unless they cause pain, they are ignored. The same logic applies to many fibular avulsions. The body reaches a state of equilibrium. The injury is resolved, even if the anatomy is altered.
Risk Factors for True Non-Union
While avulsion fractures often resolve without bony union, other fractures fail to heal due to external factors. This is called pathological non-union. If you are worried about your bone not healing, check these common culprits:
- Smoking: Nicotine constricts blood vessels, reducing oxygen delivery to the fracture site. Smokers have a significantly higher rate of non-union compared to non-smokers.
- Diabetes: High blood sugar impairs immune function and circulation, slowing down the inflammatory phase necessary for bone repair.
- Malnutrition: Bones need protein, calcium, vitamin D, and vitamin C. A deficient diet lacks the building blocks for new bone matrix.
- Movement: Excessive motion at the fracture site prevents the delicate web of new bone (callus) from forming. Think of it like trying to build a sandcastle while someone keeps kicking the bucket.
If you have any of these conditions, your doctor will monitor your healing closely. They might use electrical stimulation or bone grafts to jumpstart the process. But for the average healthy person with a simple avulsion fracture, patience is the only prescription needed.
Diagnostic Clues: How Doctors Know
How do you know if your bone is healing or stuck? Pain is a poor indicator. Inflammation can persist for months. Imaging is key.
X-rays show the gross anatomy. If the gap between bone fragments hasn’t narrowed after six months, it’s a sign of trouble. CT scans provide a 3D view, revealing whether any microscopic bridging is occurring. MRI is the gold standard for assessing soft tissue and bone marrow edema. If the marrow signal remains high (bright on T2 images), the bone is still stressed and attempting to heal. If the signal drops out, the bone may be dead or simply accepted as a non-union.
Doctors also look for "hypertrophic" vs. "atrophic" non-unions. Hypertrophic means there is plenty of callus formation, but the bone ends aren't touching-usually a mechanical problem. Atrophic means there is no callus at all-a biological problem, often due to poor blood supply or systemic illness.

Treatment Options for Stubborn Bones
If a bone truly fails to heal and causes pain, options exist. Conservative care involves rest, bracing, and physical therapy to strengthen surrounding muscles. If that fails, surgery is considered.
Surgical interventions include:
- Debridement and Compression: Cleaning out dead tissue and screwing the bone ends together tightly.
- Bone Grafting: Taking healthy bone from the pelvis or using synthetic substitutes to fill the gap and stimulate growth.
- Electrical Stimulation: Using low-intensity currents to encourage osteoblasts (bone-building cells) to work faster.
- Removal: In the case of painful loose bodies, like a symptomatic fibular fragment, surgeons may simply remove the piece entirely.
For the classic fibular avulsion, removal is rare. Usually, time and rehab are sufficient. The body is remarkably good at compensating for minor structural imperfections.
Living With a Non-Union
Can you live a normal life with a bone that never healed? Absolutely. Many athletes return to competition with documented non-unions. The key is managing expectations. Your bone might not look perfect on an X-ray, but if it functions well, it is fine.
Physical therapy plays a huge role here. Strengthening the muscles around the injured area takes pressure off the bone. For ankle injuries, balance training is crucial. Proprioception-the body's ability to sense its position in space-is often impaired after injury. Rebuilding this neural connection helps prevent re-injury, regardless of the bone's status.
Dietary adjustments can also support long-term bone health. Adequate protein intake supports collagen synthesis, the scaffold upon which bone mineralizes. Vitamin K2 helps direct calcium to the bones rather than the arteries. These aren't cures for non-union, but they optimize the environment for whatever healing potential remains.
Conclusion: Redefining Healing
The question "Which bone never heals?" is a trick question. No bone is inherently doomed to failure. However, the fibula, particularly in avulsion fractures, often serves as a testament to the body's pragmatic approach to injury. It chooses function over form. It accepts a permanent change in anatomy if it means preserving mobility and minimizing pain.
Understanding this distinction empowers patients. You don't need to panic if your X-ray shows a gap. Ask your doctor: "Is this functional?" If the answer is yes, then the healing process, in the broadest sense, is complete. The bone may not be united, but you are whole.
Does the fibula ever fully heal after an avulsion fracture?
Often, no. Small avulsion fragments of the fibula may remain permanently detached. However, this is usually not a problem. The tendon heals via scar tissue, restoring function without the need for bony union. Patients typically recover full mobility without issues.
What is the difference between a non-union and malunion?
A non-union means the bone fragments have failed to join together at all. A malunion means the bone has healed, but in the wrong position or alignment. Malunions can cause arthritis or mechanical issues later, while non-unions may be asymptomatic if stable.
Why does the scaphoid bone have trouble healing?
The scaphoid has a unique retrograde blood supply. Blood enters from the distal end and flows backward. Fractures near the proximal pole can cut off blood flow to the larger fragment, leading to avascular necrosis (bone death) and preventing healing.
Can smoking prevent a bone from healing?
Yes. Smoking is one of the biggest risk factors for non-union. Nicotine restricts blood vessels, reducing oxygen and nutrient delivery to the fracture site. Quitting smoking significantly improves the chances of successful bone repair.
When should I see a doctor for a suspected non-union?
If you continue to experience pain, swelling, or instability at the fracture site after three to six months, consult an orthopedic specialist. Persistent symptoms suggest that the bone may not be healing correctly and may require further intervention.