Quick Takeaways
- Health outcomes vary more by socioeconomic and lifestyle factors than by race alone.
- Major diseases such as Cardiovascular disease are leading causes of death across all racial groups show distinct prevalence patterns.
- Genetic predispositions exist, but they interact heavily with environment, diet, and access to care.
- Medical tourism can give patients access to specialized treatments not available in their home country, but it does not change underlying racial health trends.
- Focusing on modifiable risk factors-diet, exercise, smoking, stress-yields the biggest health gains for any group.
Understanding the Question: What Does “Healthiest Race” Mean?
When people ask “what is the healthiest race?”, they usually mean: which ethnic group, on average, lives the longest or suffers the fewest chronic diseases? The answer isn’t simple, because health is a blend of genetics, environment, culture, economics, and public policy. To untangle the web, we need to look at three layers:
- Genetic risk factors that differ among populations.
- Behavioural and lifestyle patterns that shape disease risk.
- Socio‑economic conditions that dictate access to preventive care.
Only by examining all three can we avoid the trap of stereotyping and instead focus on evidence‑based strategies.
Genetic Influences: Real Differences, Limited Impact
Scientific research has identified several genetic variants that are more common in certain groups. For example, the APOE‑ε4 allele is linked to higher Alzheimer’s risk and appears more frequently in people of African descent. Conversely, the SLC30A8 gene variant is associated with lower type‑2 diabetes risk and is more prevalent among East Asian populations.
These genetic clues matter for personalized medicine, but they explain only a fraction of observed health gaps. Even when a variant raises risk, lifestyle can offset it. For instance, many Japanese Americans carry the diabetes‑protective allele, yet a shift toward Western diets has increased diabetes rates in that community.
Behavioural and Lifestyle Factors
Diet, physical activity, smoking, and alcohol use differ sharply across cultures and directly affect major disease burdens. Below are a few contrasting examples:
- Diet: Traditional Mediterranean diets, rich in olive oil, fish, and vegetables, are common among Southern Europeans and correlate with lower Cardiovascular disease rates. In contrast, high‑salt, high‑processed‑food diets in some South Asian communities contribute to higher hypertension prevalence.
- Physical activity: Rural African populations often engage in more daily physical labour, resulting in lower obesity rates compared with urbanized groups.
- Smoking: Cigarette consumption remains highest in Eastern Europe, driving excess lung cancer and heart disease deaths.
These habits are modifiable. Public health programs that promote healthier eating and regular exercise have repeatedly narrowed the gap between groups.

Socio‑Economic and Healthcare Access
Income, education, and health insurance coverage are the strongest predictors of life expectancy. In the United States, for example, the average life expectancy for non‑Hispanic White adults with a college degree exceeds 80 years, while for non‑Hispanic Black adults without a high school diploma it drops below 70 years. These disparities dwarf any genetic differences.
Access to preventive services-screenings, vaccinations, prenatal care-also varies. Countries with universal health coverage, such as Japan or Sweden, see relatively small health gaps among ethnic minorities, underscoring the power of systemic support.
Comparing Major Diseases Across Four Broad Racial Groups
| Racial/Ethnic Group | Cardiovascular disease (%) | Diabetes (%) | Obesity (BMI ≥ 30) (%) | Hypertension (%) | Cancer (all sites) (%) |
|---|---|---|---|---|---|
| European descent (Caucasian) | 7.5 | 6.0 | 22 | 28 | 24 |
| East Asian | 5.2 | 4.5 | 5 | 20 | 18 |
| African descent | 8.1 | 7.8 | 14 | 30 | 22 |
| Hispanic/Latino | 6.8 | 9.0 | 12 | 25 | 19 |
These numbers are averages drawn from World Health Organization and CDC databases. They illustrate that while certain groups have higher rates of specific diseases, no single race is universally “healthy”.
Medical Tourism: Does It Shift the Health Landscape?
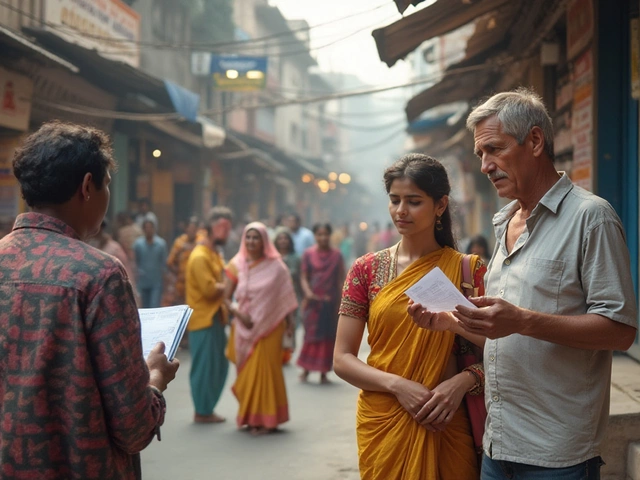
People often wonder if traveling abroad for treatment can improve health outcomes for groups that traditionally fare worse. Medical tourism offers elective surgeries, fertility services, and specialized chronic‑disease care at lower costs does provide access to procedures that might be delayed at home, but it doesn’t alter the root causes of racial health disparities.
For example, a patient from a low‑income African background might travel to India for a cardiac bypass at a fraction of the UK price. The surgery can save lives, yet the underlying risk factors-high blood pressure, diet, stress-remain unless addressed through long‑term lifestyle changes.
Moreover, medical tourism introduces new challenges: follow‑up care gaps, language barriers, and variable quality standards. Choosing accredited facilities and ensuring continuity with local physicians are essential safeguards.

Practical Takeaways: How Any Group Can Boost Health
Regardless of genetic background, the following evidence‑based steps yield measurable health gains:
- Adopt a plant‑forward diet: Aim for at least five servings of fruits and vegetables daily, reduce red meat, and limit sugary drinks.
- Stay active: 150 minutes of moderate aerobic activity per week (walking, cycling) plus muscle‑strengthening twice a week.
- Control blood pressure: Monitor regularly, keep sodium intake under 2,300 mg, and manage stress through meditation or hobbies.
- Get screened: Regular checks for cholesterol, blood sugar, and cancers appropriate to age and family history.
- Prioritize sleep: 7‑9 hours nightly supports metabolism and immune function.
Health systems can amplify these gains by offering community‑based education, affordable screenings, and culturally sensitive counseling.
Frequently Asked Questions
Is there any race that consistently lives longer than others?
Life expectancy varies more by country, income level, and healthcare access than by race. In high‑income nations, Japanese and other East Asian populations often show the highest averages, but that reflects diet, social structure, and universal health coverage rather than genetics alone.
Do genetics determine who gets sick?
Genetics set a baseline risk, but environmental factors usually decide whether disease actually develops. For most chronic conditions, lifestyle and healthcare access outweigh genetic predisposition.
Can medical tourism improve my health outcomes?
It can provide timely, affordable procedures that might otherwise be delayed, but it does not replace the need for ongoing preventive care, medication adherence, and lifestyle management when you return home.
What are the biggest modifiable risk factors for all races?
Tobacco use, unhealthy diet, physical inactivity, excessive alcohol, and uncontrolled hypertension are the top contributors to premature death across any ethnic group.
How can governments reduce racial health gaps?
Invest in universal primary‑care coverage, fund community health worker programs in underserved neighborhoods, regulate food marketing, and ensure equitable access to quality education and housing.
Bottom Line
There isn’t a single “healthiest race”. Health is shaped by a mix of genes, daily habits, and the social environment. By targeting the factors we can change-nutrition, activity, preventive care-we can improve outcomes for every community. Whether you’re considering a treatment abroad or simply want to live longer, focus on the actions within your control and push for policies that level the playing field for all.